Beyond the 'Pee Phenomenon': The Physiology of Immersion Diuresis and Dive Safety
Every diver knows the feeling. You’ve barely finished your descent, settled into your buoyancy, and started admiring the reef when it hits: the unmistakable, urgent need to urinate. In the dive community, we often joke about "breaking the seal" or the warmth of a wetsuit on a cold day, but this isn't just a minor inconvenience or a lack of bladder control. It is a complex physiological response known as immersion diuresis.
While the "pee phenomenon" is often treated as a punchline, for the technical and advanced diver, it represents a significant physiological shift with direct implications for safety. Understanding why your body decides to jettison fluids the moment you hit the water is critical for managing hydration, gas kinetics, and your overall risk of decompression sickness (DCS).
The Physics of Pressure: Hydrostatic Force as the Catalyst
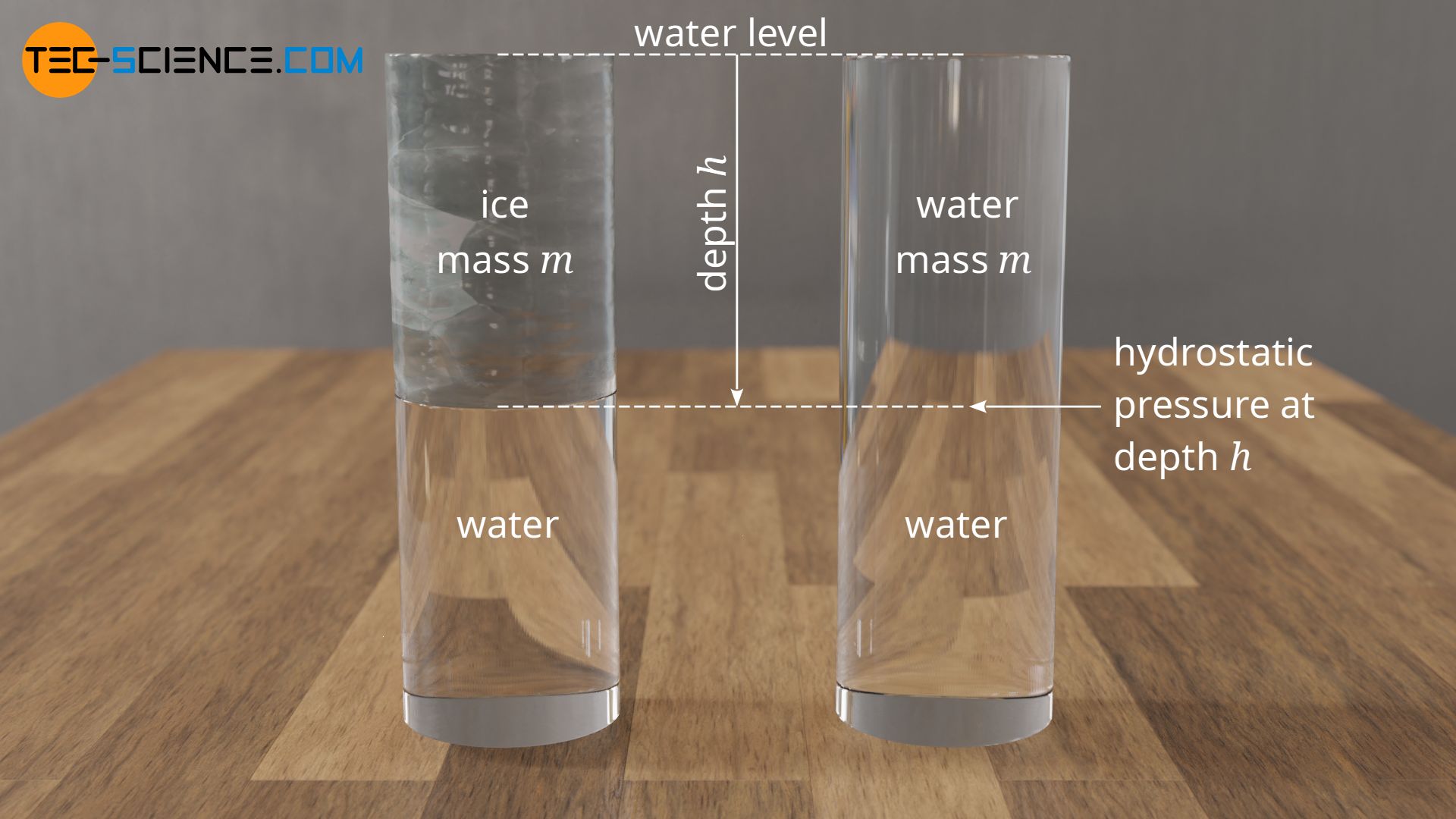
The process begins the moment you submerge. Unlike air, water is a dense medium that exerts significant hydrostatic pressure on the body 1. Because water is approximately 800 times denser than air, it exerts a uniform, inward force on every square inch of your skin 1.
As you descend, this pressure acts on the peripheral soft tissues and the superficial veins in your extremities. Even at shallow depths, the hydrostatic pressure is sufficient to compress these vessels. Because the veins in your arms and legs are more compliant (stretchable) than the arteries, they are easily squeezed, pushing the blood they contain toward the only area of the body that isn't being compressed in the same way: the thoracic cavity (the chest).
The Thoracic Blood Shift: Centralizing Your Volume
This movement of fluid is known as the thoracic blood shift. Under the influence of hydrostatic pressure, a significant volume of blood—estimated at 500ml to 700ml—is forced from the limbs into the heart and lungs 2.
This creates a physiological paradox. Your total blood volume hasn't actually increased, but your "central" blood volume has. Your heart and the large vessels in your chest perceive this influx as an over-hydration event. This triggers the Gauer-Henry Reflex, a sensor-based mechanism that tells the body it has too much fluid in circulation.
The body’s primary concern is maintaining a stable internal environment. When the stretch receptors in the right atrium of the heart detect this increased volume, they interpret it as a signal that the blood pressure is too high and must be lowered immediately.
The Hormonal Cascade: ANP, BNP, and ADH Suppression
To correct this perceived fluid overload, the body initiates a rapid hormonal response. This is where the "urge" truly begins.
- Atrial Natriuretic Peptide (ANP): The stretching of the heart’s atrial walls triggers the release of ANP. This hormone acts directly on the kidneys to increase the excretion of sodium and water.
- B-type Natriuretic Peptide (BNP): Similar to ANP, this peptide is released from the ventricles and further encourages the kidneys to dump fluid.
- Anti-Diuretic Hormone (ADH) Suppression: Normally, the pituitary gland releases ADH (also known as vasopressin) to tell the kidneys to retain water. During immersion, the brain suppresses ADH production. Without ADH, the "floodgates" of the kidneys open, allowing water to pass into the bladder at an accelerated rate.
This chemical cocktail is a biological "pressure valve." The body is effectively trying to urinate away its perceived excess blood volume to protect the heart from over-pressurization.
Kidney Filtration: The Biological Pressure Valve
Once the hormonal signals reach the kidneys, the Glomerular Filtration Rate (GFR)—the speed at which your kidneys process blood—increases significantly. Immersion diuresis is not a slow, steady process like standard hydration; it is an aggressive, rapid-fire response.
Crucially, this isn't just water loss. It is also natriuresis, the loss of essential electrolytes, specifically sodium. This is why post-dive fatigue is often more than just physical exertion; it is a result of a literal chemical imbalance caused by the rapid processing of fluids and salts.
| Process | Mechanism | Result |
|---|---|---|
| Vasoconstriction | Cold/Pressure narrows peripheral vessels | Blood moves to core |
| Atrial Stretch | Central volume increases | ANP/BNP hormones released |
| ADH Suppression | Pituitary stops "water-saving" signal | Kidney filtration increases |
| Diuresis | Kidneys excrete water and salt | Bladder fills; blood thickens |
The Decompression Connection: Fluid Loss and Gas Kinetics
This is where immersion diuresis moves from an inconvenience to a safety risk. As the kidneys dump water, the remaining blood in your circulatory system becomes more concentrated. This is known as hemoconcentration.
When blood loses its plasma volume, it becomes more viscous (thicker). This change in "sludge factor" has a profound impact on how your body handles inert gases like nitrogen or helium.
Hemoconcentration and Kinetic Asymmetry
We have previously discussed Kinetic Asymmetry, the principle that nitrogen often leaves the body slower than it enters. Dehydration caused by immersion diuresis exacerbates this problem. Thick, viscous blood moves more slowly through the capillary beds of "slow" tissues like fat and cartilage. If the blood cannot flow efficiently, it cannot pick up the nitrogen molecules that need to be transported to the lungs for exhalation.
Compromising Your M-Values
Your dive computer calculates your "invisible ceiling" based on M-values, which assume a relatively healthy, hydrated physiological state 4. If your blood is thickened by diuresis, the off-gassing models programmed into your computer may no longer reflect your actual physiological reality.
This is a primary cause of 'Undeserved' Decompression Sickness. You may follow your Gradient Factors perfectly and stay within your limits, but because your blood's ability to transport gas is compromised by fluid loss, you end up with a "hit" despite a clean profile 4.
Warning: Dehydration is one of the most significant "silent" risk factors in decompression sickness. A diver who is dehydrated at the end of a dive is essentially diving a more aggressive profile than their computer indicates.
Thermal Influence: Why Cold Water Accelerates the Urge
While hydrostatic pressure is the primary driver, temperature plays a massive supporting role. When you enter cold water, your body initiates peripheral vasoconstriction to keep your core warm. This is a survival mechanism that pulls even more blood away from your skin and limbs toward your vital organs.
This compounds the thoracic blood shift. The heart perceives an even greater volume of blood, the hormonal response is more intense, and the diuresis becomes more aggressive. This is why technical divers using helium-rich mixes often feel the urge more acutely; as explored in our piece on Thermodynamics of the Deep, helium’s high thermal conductivity strips heat from the body faster, triggering more intense vasoconstriction and, consequently, more diuresis.

Practical Management for the Advanced Diver
Understanding the "why" of immersion diuresis allows us to develop better "how" strategies for dive safety.
1. Stop 'Dry Diving'
The most dangerous mistake a diver can make is "dry diving"—purposefully avoiding water intake before a dive to prevent the need to urinate. This starts the dive in a state of pre-existing dehydration, which, when combined with the inevitable diuresis of the dive, leads to dangerously high blood viscosity during the critical decompression phase.
2. Optimal Hydration Strategies
Not all fluids are created equal. To combat both the water loss and the electrolyte loss (natriuresis), your pre-dive hydration should be focused.
- Pre-Hydrate: Drink 500ml of water/electrolyte mix 60–90 minutes before the dive.
- Isotonic over Hypotonic: Use isotonic drinks (which match the salt concentration of your blood) to ensure the fluid actually stays in your vascular system rather than just passing through.
- Avoid Diuretics: Caffeine and alcohol increase ADH suppression, making the "pee urge" even worse.
3. Managing the Inevitable
On long-duration technical dives, you must have a plan for relief.
- P-valves: For drysuit divers, a P-valve is a critical piece of safety equipment, not just a luxury. It allows for hydration throughout the dive without discomfort.
- Adult Diapers: For many female technical divers or those in wetsuits on long deco hangs, high-absorbency diapers are a standard tool of the trade.
- Psychological Barrier:
Holding it in is a sign of toughness— actually, holding a full bladder causes stress, increases heart rate, and can distract you from critical safety checks.
4. Post-Dive Rehydration
Rehydration doesn't end when you surface. Because your blood is at its thickest during your ascent and immediate post-dive period, you should begin drinking fluids immediately upon surfacing to help flush remaining nitrogen and restore plasma volume.
Conclusion: Respecting the Biological Cost of Depth
Immersion diuresis is an unavoidable biological tax we pay for entering the underwater world. It is the result of a complex axis involving hydrostatic pressure, the Gauer-Henry Reflex, and the hormonal regulation of our kidneys 2.
By recognizing that this process begins the moment we submerge, we can move beyond the jokes and treat hydration as a core component of our decompression theory. Safety isn't just about the gas in your tanks or the settings on your computer; it’s about the state of the "biological machine" doing the diving.
Next time you feel that familiar urge underwater, remember: your body is reacting to the physics of the deep. Respect that reaction, stay hydrated, and give your circulatory system the fluid it needs to bring you home safely.