Spinal Cord Pathophysiology: Why the CNS is Uniquely Vulnerable to Rapid Pressure Shifts
In the world of technical and advanced recreational diving, we often talk about "the bends" as a singular boogeyman. We visualize joint pain or perhaps a skin rash, but the reality of decompression sickness (DCS) is far more nuanced and, in its most severe forms, significantly more dangerous. When we move beyond the musculoskeletal aches of Type I DCS, we enter the realm of Type II DCS—a category defined by its assault on the central nervous system (CNS). 2
The spinal cord is the primary theater for these high-stakes neurological incidents. While the brain is occasionally involved, the spinal cord remains uniquely vulnerable to the physics of rapid pressure shifts. Understanding the pathophysiology of the spinal cord is not just an academic exercise; it is a fundamental requirement for any diver looking to manage the risks of deep, repetitive, or decompression-intensive diving. This vulnerability stems from a perfect storm of high lipid content, unique vascular structures, and the mechanical reality of bubbles forming directly within delicate neural pathways. 13
The Lipid-Rich Environment: Myelin as a Nitrogen Sponge
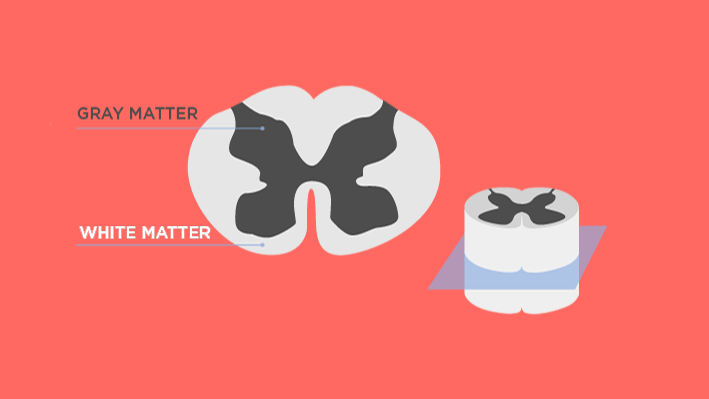
To understand why the spinal cord is a target, we must first look at its chemical composition. The CNS is largely composed of white matter and gray matter. The white matter, in particular, is densely packed with myelin—a fatty substance that wraps around axons to insulate electrical impulses. This high lipid content makes the spinal cord a literal sponge for nitrogen. 3
According to the Meyer-Overton Hypothesis, the narcotic potency and solubility of a gas are directly related to its lipid solubility. Nitrogen is highly soluble in fats, meaning that during the loading phase of a dive, the lipid-rich tissues of the spinal cord absorb a significant volume of inert gas.
However, the spinal cord presents what we call the "slow-tissue paradox." While it has a high capacity for nitrogen storage due to its lipid content, its blood supply is relatively sparse compared to the highly vascularized gray matter of the brain. 3 This creates a situation where the cord loads up on nitrogen during the dive but struggles to "off-gas" efficiently during ascent. As the surrounding ambient pressure drops, the white matter remains saturated, creating the ideal conditions for supersaturation and subsequent bubble formation.
The Batson Venous Plexus: A Vascular Vulnerability
The way blood leaves the spinal cord is just as critical as how it arrives. Most of the body’s venous systems utilize one-way valves to ensure blood flows toward the heart. The spinal cord, however, utilizes a unique network known as the Batson Venous Plexus. This is a system of epidural veins that is entirely valveless. 3
Because there are no valves, the direction of blood flow in this plexus is determined entirely by pressure gradients. This creates several specific risks for divers:
- Retrograde Flow: Activities that increase thoracic pressure—such as a forceful Valsalva maneuver to clear the ears, heavy lifting, or even coughing—can momentarily reverse the flow of blood. If a diver has "silent" venous bubbles in their systemic circulation, these bubbles can be pushed backward into the spinal venous system.
- The Stagnant Zone: The lack of valves, combined with the low-pressure nature of the plexus, can lead to "stagnant" venous drainage. When bubbles enter this system, they can cause venous congestion, effectively "clogging" the exit for deoxygenated blood.
- Venous Infarction: As bubbles accumulate in the Batson Plexus, they block the outflow of blood from the cord. This leads to a backup of pressure, causing a venous infarction—where the tissue dies not because it didn't get oxygenated blood, but because the "used" blood had nowhere to go. 3
| Feature | Systemic Veins | Batson Venous Plexus (Spinal) |
|---|---|---|
| Valves | Present | Absent |
| Flow | Unidirectional | Bi-directional (Pressure-based) |
| Risk | Filtered by Lungs | Susceptible to Retrograde Bubbles |
| DCS Role | Type I Symptoms | Type II Spinal Cord Injury |
Autochthonous Bubble Formation: Damage from Within
While many divers focus on bubbles traveling through the bloodstream (intravascular), the spinal cord is frequently damaged by autochthonous bubbles. These are bubbles that form in-situ, directly within the tissue itself. 23
When the nitrogen-saturated lipids of the spinal white matter undergo rapid decompression, the gas can come out of solution so quickly that it forms bubbles inside the myelin sheath and between the nerve fibers. The results are mechanically catastrophic:
- Mechanical Shearing: As the bubble expands, it physically tears and stretches the delicate axons. This disrupts the electrical signals traveling between the brain and the body. 3
- Tissue Distension: The physical presence of the bubble increases internal tissue pressure, which can shut down local capillary blood flow, leading to localized hypoxia (oxygen starvation). 3
- BSCB Disruption: The mechanical stress can break down the Blood-Spinal Cord Barrier (BSCB), allowing inflammatory proteins and fluids to leak into the neural tissue, causing swelling (edema) that further compresses the nerves.
The Inflammatory Cascade and Ischemic Injury
The damage from a decompression hit doesn't stop once the bubbles stop growing. The body treats a bubble as a foreign invader, triggering a complex biochemical war known as the inflammatory cascade. 2
When bubbles form, they damage the endothelial lining of the blood vessels. This damage activates leukocytes (white blood cells) and platelets, which rush to the site and begin to clump together. The blood becomes "thicker" and more prone to clotting, a process that can continue for hours after the diver has reached the surface. 2
This leads to ischemia-reperfusion injury. Even if a diver is recompressed and the bubbles are shrunk, the secondary inflammatory damage—swelling, clotting, and the release of free radicals—can continue to kill spinal neurons. This is why "unusual fatigue" after a dive is often a sign of systemic biochemical stress. 4
Furthermore, the presence of excess CO2 can exacerbate this process. As explored in our guide on CO2 retention and skip breathing, high levels of carbon dioxide act as a potent vasodilator in the CNS, potentially increasing the delivery of inert gas to the cord during the dive and complicating the recovery phase.
PFO and the Shortcut to the Cord
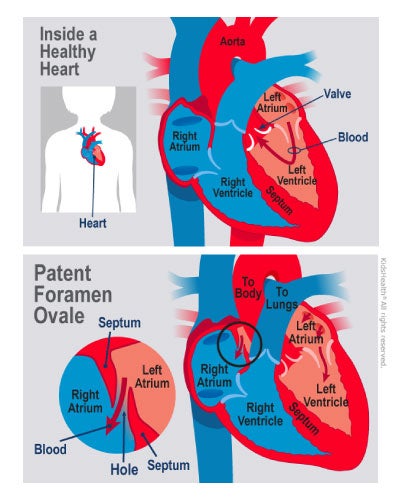
For some divers, spinal DCS occurs even when they follow their dive computers perfectly—a phenomenon known as an "undeserved" hit. A common culprit in these cases is a Patent Foramen Ovale (PFO). 3
A PFO is a small hole between the right and left atria of the heart. Under normal conditions, the lungs act as a filter, trapping small venous bubbles and allowing them to be exhaled. However, if a diver has a PFO, a pressure spike (like a Valsalva or a hard kick) can cause blood to shunted from the right side of the heart to the left, bypassing the pulmonary filter entirely. 3
Once these bubbles enter the arterial side, they have a direct route to the spinal cord's arterial supply. This turns what would have been harmless "silent" venous bubbles into dangerous arterial gas emboli (AGE). You can read more about this mechanism in our detailed breakdown of PFO and 'undeserved' DCS.
Clinical Presentation: Why Symptoms Ascend
Recognizing spinal DCS early is critical for a positive outcome. Unlike the localized pain of a "bent" elbow, spinal symptoms often follow a predictable and terrifying progression.
The Diver's Girdle
One of the earliest warning signs of spinal cord involvement is a sensation of tightness or pain around the midsection, often called the "girdle" sensation. This is frequently followed by paresthesia (pins and needles) or numbness in the lower extremities. 4
Ascending Paralysis
Because the spinal cord is a vertical highway of information, damage to a specific segment can cut off everything below it. Symptoms often "ascend"—starting with weakness in the toes or feet and moving up the legs to the hips. If left untreated, this can progress to full paralysis and loss of bladder/bowel control. 4
Expert Warning: It is vital to distinguish spinal DCS from other neurological issues. While oxygen toxicity typically presents with localized muscle twitching or full-body convulsions (the Paul Bert Effect), spinal DCS is characterized by a loss of sensation or motor function that persists and often worsens over time. 4
Mitigating Risk: Advanced Decompression Strategies
Knowing the vulnerability of the spinal cord allows us to tailor our diving habits to protect it. It is not enough to simply "not go into deco"; we must manage the way we decompress.
1. Conservative Gradient Factors
Modern dive computers allow you to adjust Gradient Factors (GF). For high-lipid tissues like the spinal cord, using a conservative "GF Low" (e.g., 30 or 35) can help trigger deeper stops that slow the initial ascent, while a conservative "GF High" (e.g., 70 or 75) ensures you spend more time off-gassing near the surface.
2. The Final 6 Meters (20 Feet)
The greatest relative pressure change occurs near the surface. A rapid ascent from 6 meters to the surface is a common trigger for autochthonous bubble formation in the cord.
- Slow your ascent rate to 1-3 meters (3-10 feet) per minute in the final 6 meters.
- Extend your safety stop or final deco stop beyond the minimum requirements.
- Avoid physical exertion (like hauling heavy gear onto a boat) immediately after surfacing.
3. Hydration and Thermal Management
Dehydration reduces blood volume and increases blood viscosity, making the "sludging" of the inflammatory cascade much worse. Similarly, being cold during the decompression phase reduces peripheral circulation, trapping nitrogen in those "slow" lipid tissues. 4
Conclusion: Respecting the CNS in Dive Planning
The spinal cord is a masterpiece of biological engineering, but it was never designed to handle the rapid gas expansion inherent in scuba diving. Its fatty composition, unique valveless drainage, and susceptibility to internal bubble formation make it the most vulnerable part of a diver's anatomy. 1
As intermediate and advanced divers, our goal is to move beyond "following the bubbles" on a screen. By understanding the underlying pathophysiology—from the Meyer-Overton Hypothesis to the mechanics of the Batson Plexus—we can make informed decisions that prioritize the long-term health of our central nervous system. Rigorous decompression discipline, conservative surfacing habits, and an awareness of secondary injury markers are the hallmarks of a truly expert diver.
Respect the cord, manage your ascent, and never ignore the "girdle" of a potential hit. Safe diving is a product of physiological knowledge and the discipline to apply it.
Ready to dive deeper into the science of safety? Explore our guide on Heart Rate Variability and Decompression Stress to see how your body recovers from the pressures of the deep.